by Dr Sandeep Moolchandani, MBBS MHA PAHM
Hospitals form an important arm of the healthcare delivery system. Though the focus of various National programmes may be on primary health but secondary and tertiary public hospitals form one of the largest expenditure category in the national health budget. Over the past decade, inspite of the complexity of hospitals having increased many fold, not many changes have been made in the management structure of public hospitals.
It is very well known that hospitals should be hundred percent clean and hygienic, but in practice government hospitals are generally the filthiest places. Even central level tertiary government hospitals are run on primitive principles; problems of poor governance and administration is not a hidden fact. Waiting times in government hospitals can reach upto two hours just for accessing outpatient services.
Lack of governments’ commitment towards quality assurance in government setups, low management capacities at health facilities, lack of policies and guidelines from the State, as well as structural problems of the centralized health system are key problems in Public Health Sector leading to inefficient use of scarce resources and deficiencies in the quality of services provided (Davey, 2006)
This post enumerates the reasons why the public hospitals should start focusing upon delivering optimum quality of services.
1. Public Hospitals impose significant opportunity costs to the society
The secondary and tertiary care as such has a limited impact on the population health. Inspite of this known fact a major chunk of healthcare budget is spent on secondary and tertiary care which can be upto 40-50% of state healthcare budgets. Thus infrastructure and administrative costs of hospitals carry a big opportunity costs with them.
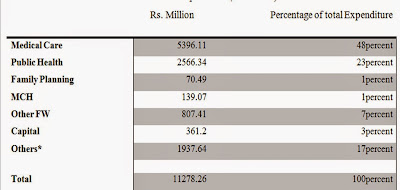 |
| Maharashtra 2000-01 Public Health Expenditure (Rs. Million) in Urban Areas |
In 2000-01, 48percent of public health expenditure in Maharashtra, which amounts to Rs 5396.11 million, was incurred on medical care alone.
2. Decreasing utilization of Public Hospitals for Inpatient and Outpatient Care
Some studies on the patterns of utilization of health care facilities indicate that the private health care provider is preferred for the cost and quality of the health care services provided (Uplekar 1989a, 1989b; Viswanathan and Rohde 1995).
80percent of households prefer to use private sector treatment in India for minor illnesses, and 75percent of households prefer to go to the private sector for major illnesses (M.Uplekar, V.Pathania, & M.Raviglione). Numerous other studies have confirmed the dominance of the private sector and the reasons for this dominance: government health services entailed longer waiting periods, arrogant behaviour of doctors and non-availability of medicines (Ananthakrishnan). Even though the treatment in public hospitals is free, the patients have to pay for tests, and bear the incidental costs of boarding and lodging (Pasricha, 2006).
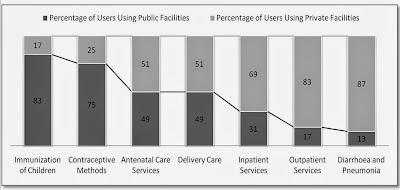 |
| Chart: Sources of Utilization of Health Care Services, Maharashtra (Adapted from “Health And Healthcare In Maharashtra: A Status Report”, Ravi Duggal, 2005) |
The users don’t prefer to use public facilities for medical services like Inpatient and Outpatient services in contrast to other primary healthcare services especially in urban setup as per the data published by National Sample Survey Organization (NSSO). The major public providers which provide these services in urban setups are teaching hospitals and general hospitals. There is a clear preference towards private providers despite of costly treatments in secondary and tertiary domain. This data points towards the failure of public hospitals in meeting the expectations of the public.
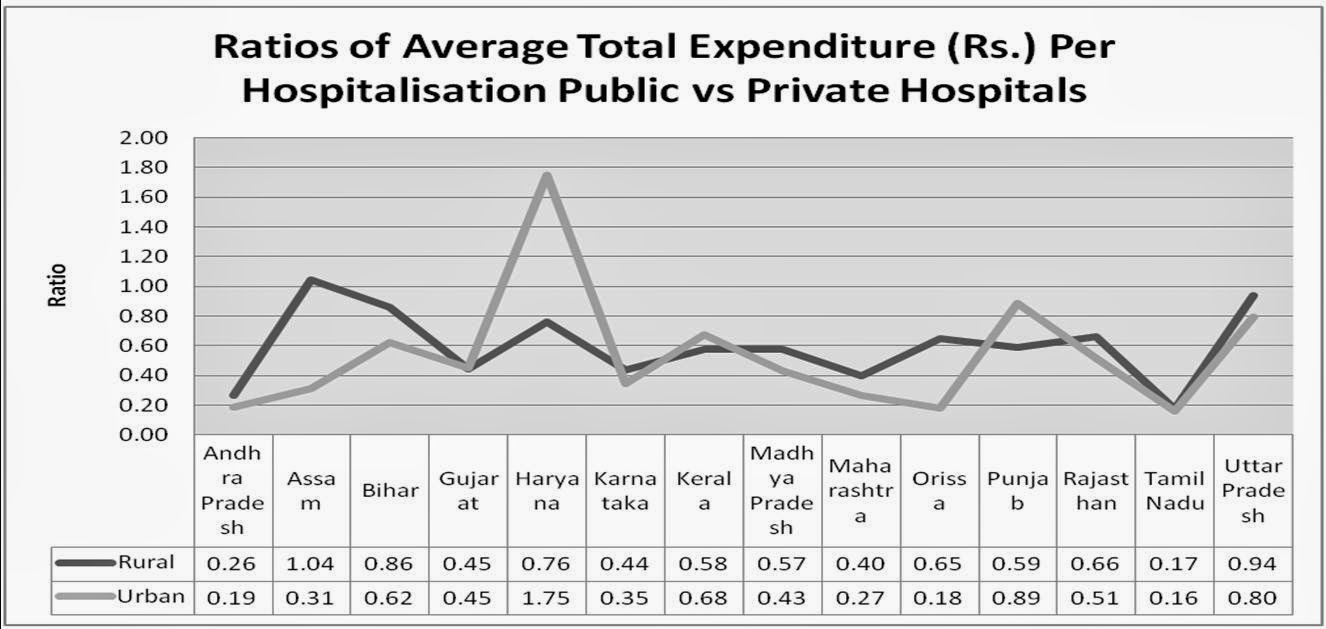
3. Health Expenditure incurred by patients in Public Hospitals vs Private Hospitals
The ratio of hospitalisation expenditures in public vs private hospitals in urban setups ranges between 0.16 in Tamil Nadu to 1.75 in Haryana. The services provided in public hospitals amount to a considerable fraction of the costs in private hospital. Even after spending a comparable amount, all patient gets is dismal sanitary conditions, long waiting times, rude behaviour of staff, high infection rates and substandard clinical care. This is one of the prominent reasons why the patients prefer private healthcare providers more than public hospitals.
A significant dilemma is faced by middle income groups who can spend on healthcare but not as much as charged in good private tertiary setups; while in case of treatments in government hospitals the quality of services provided is too bad to meet their expectations. The middle class comprises to around 25 to 30 percent of the total population of India.
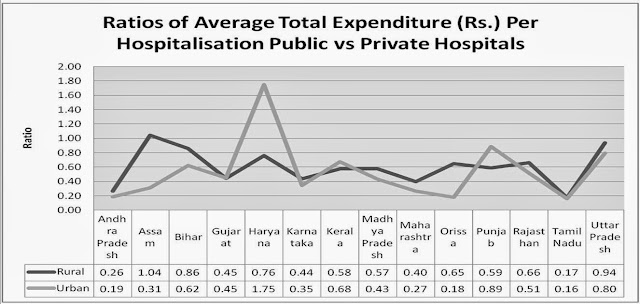 |
| Major State-wise Average Total Expenditure (Rs.) Per Hospitalisation by Type of Hospital for Rural and Urban Areas in India |
There are three things which should be clear with respect to the treatment in a government hospital, firstly the treatment in government hospitals is not completely free, secondly apart from these costs there are costs involved due to loss of daily livelihood and thirdly there are potential costs that can come into picture due to bad quality of treatment (improper instructions while prescribing, post op infections, medical errors, medical negligence etc).
Conclusion
A significant amount of taxpayer’s money is spent on Government hospitals which puts these hospitals in a critical position to be accountable for the quality of services and deliver quality services within the constraints of available resources. It should be tried by the public hospitals to prevent diversion of its customer to private setups due bad quality of services. This warrants an existence of a quality management and control mechanism for government hospitals.
Quality of service should not be denied just because the direct consumer is not asking for it; but concrete measures towards quality assurance are necessary because lots of money is being spent in providing the infrastructure and bearing the administrative costs in the public hospitals. A few state governments (Gujarat, Kerala) are coming up with answers to these questions by taking concrete actions towards quality assurance and commitment for continuous quality improvement.
References:
- Duggal, R., Dilip, T. R., & Raymus, P. (2005). HEALTH AND HEALTHCARE IN MAHARASHTRA: A Status Report. Mumbai: CEHAT.
- Davey, D. A. ( 2006, June). Central Beaureau of Health Intelligence. Retrieved Feb 2011, from Health Sector Policy Reform Options Database (HS-PROD).
- M.Uplekar, V.Pathania, & M.Raviglione. Private practitioners and public health: weak links in tuberculosis control. The Lancet , Volume 358 (Issue 9285), Pages 912-916.
- Rhode, Jon Eliot and Hema Viswanathan (1995) The Rural Private Practitioner, Delhi, Oxford University Press.
- Ananthakrishnan, G. (n.d.). 75% prefer the private sector . Retrieved May 3rd, 2010, from Infochange Agenda: http://infochangeindia.org/20050604394/Agenda/Access-Denied/75-prefer-the-private-sector.html
- Jayesh P. Aagja, Renuka Garg, (2010) “Measuring perceived service quality for public hospitals (PubHosQual) in the Indian context”, International Journal of Pharmaceutical and Healthcare Marketing, Vol. 4 Iss: 1, pp.60 – 83